Key Takeaway
Medical urine bag weighing replaces manual measurement with continuous, automated weight-based monitoring of urine output. A micro load cell (typically 1–10 kg capacity) suspends the urine bag and converts real-time weight into an electrical signal, which is digitized and converted to volume using urine density (~1.020 g/mL). GALOCE's GML611 (1–50 kg, aluminum, 80×12.7×12.7 mm) and GML670 (5–200 kg, manganese steel, 34 mm) provide the precision (±0.05% F.S.), compact footprint, and long-term stability required for ICU, CCU, and operating room environments.
Why Urine Output Monitoring Matters
Urinary flow rate is an important indicator reflecting the dynamic balance of body fluids and the function of the heart and kidneys. Accurate monitoring of urine volume helps clinicians assess changes in a patient's condition and guide treatment plans — including fluid resuscitation, diuretic dosing, and early detection of acute kidney injury (AKI).
For critically ill patients in the ICU, CCU, and operating rooms, urine output monitoring has advanced from shift-based measurement to hourly or even minute-by-minute observation. Key clinical thresholds that demand real-time data include:
|
Clinical Scenario
|
Monitoring Target
|
Why Real-Time Matters
|
|
Acute Kidney Injury (AKI)
|
Oliguria <0.5 mL/kg/h
|
Early detection enables RRT initiation before irreversible damage
|
|
Fluid Resuscitation
|
Output vs. input balance
|
Prevents hypervolemia (pulmonary edema) or hypovolemia (shock)
|
|
Post-Operative Recovery
|
Return to normal output
|
Confirms renal function restoration after anesthesia
|
|
Sepsis / Septic Shock
|
Hourly urine output trend
|
Tracks perfusion adequacy during vasopressor titration
|
|
Dialysis / CRRT
|
Ultrafiltration volume
|
Ensures precise fluid removal targets are met
|
Limitations of Traditional Measurement Methods
In current clinical practice, nurses typically measure and record patients' urinary flow rate using measuring cups or graduated urine bags. While this approach has been used for decades, it suffers from significant limitations:
|
Limitation
|
Impact on Patient Care
|
Weight-Based Solution
|
|
Manual reading errors
|
Parallax, meniscus ambiguity → ±10–20% inaccuracy
|
Digital sensor eliminates human reading; ±0.05% F.S. accuracy
|
|
No real-time data
|
Hourly checks miss sudden output changes between intervals
|
Continuous monitoring with per-second updates
|
|
Labor-intensive
|
Nurses spend significant time measuring & documenting
|
Automated data logging to HIS/EMR systems
|
|
Infection risk
|
Open handling of urine bags exposes staff to pathogens
|
Closed system; no contact with fluid required
|
|
No digital integration
|
Paper records cannot feed into clinical decision support
|
RS485/USB/Wi-Fi output to hospital information systems
|
Urine dynamic monitoring has gradually become a new member of bedside monitoring devices and is widely used in Europe and America. It has been integrated into the clinical critical information systems of medical centers and has become an essential monitoring device for ICU, CCU, and operating room environments.
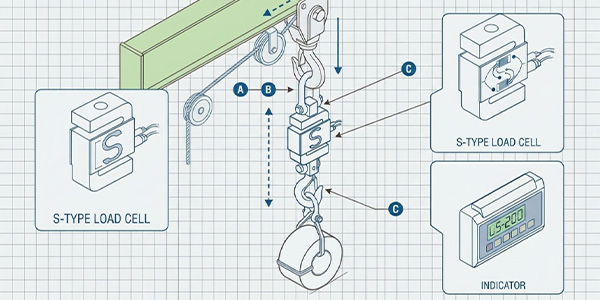
Weight-Based Urine Volume Measurement Principle
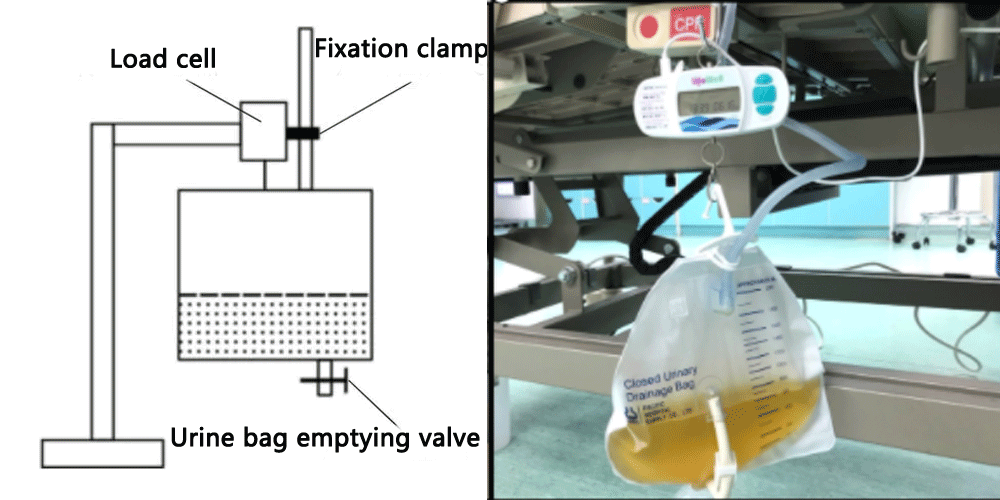
Among the various dynamic urine flow monitoring methods, the weight method has emerged as a practical and reliable approach. The core principle is simple: the urine bag is suspended from a load cell, which continuously measures the total weight of the bag and its contents. The urine volume is then calculated by converting weight to volume using the known density of urine.
The conversion formula is:
Urine Volume (mL) = [Measured Weight (g) − Tare Weight (g)] / Urine Density (g/mL)
Example: Weight reading = 2,150 g, Tare = 180 g, Density = 1.020 g/mL → Volume = (2150 − 180) / 1.020 ≈ 1,931 mL
Urine density typically ranges from 1.002 to 1.030 g/mL depending on concentration. For clinical urine output monitoring, a standard density of 1.020 g/mL is commonly used, yielding volume accuracy within ±2% — far superior to visual bag reading.
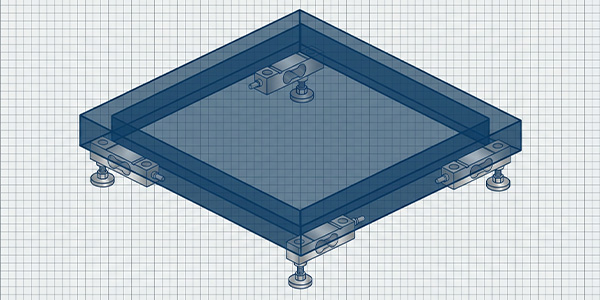
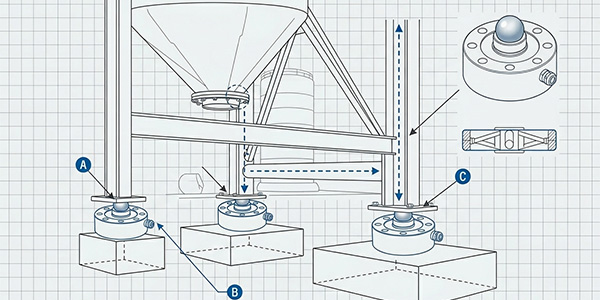
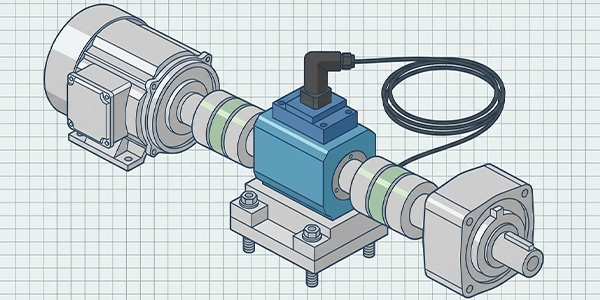
System Architecture
A complete urine bag weighing monitoring system consists of the following layers:
|
Layer
|
Component
|
Function
|
|
Sensing
|
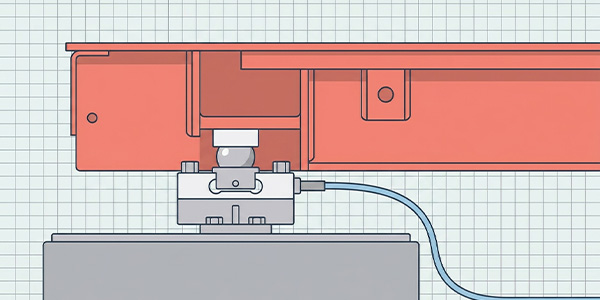
Micro Load Cell (GML611 / GML670)
|
Suspended from a bracket; supports the urine bag; converts weight to mV signal
|
|
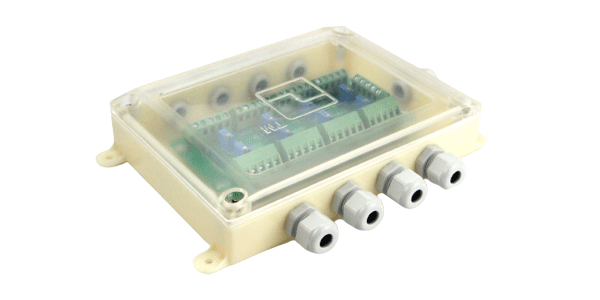
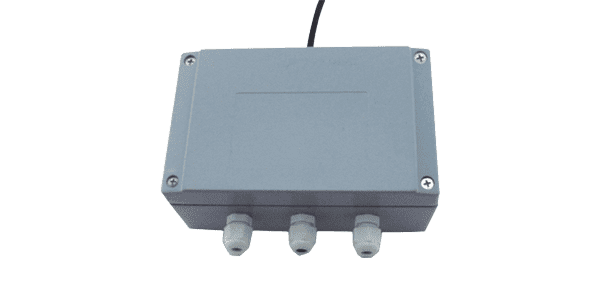
Signal Conditioning
|
A/D Converter / Transmitter
|
Amplifies and digitizes the mV signal to 24-bit digital data
|
|
Processing
|
Microcontroller (MCU)
|
Applies tare subtraction, density conversion, calculates flow rate (mL/h), triggers alarms
|
|
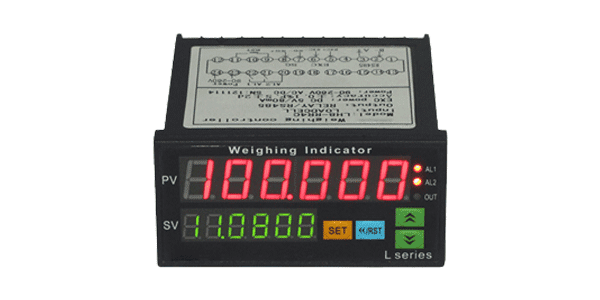
Display
|
LCD / OLED Screen
|
Shows real-time volume, flow rate, cumulative output, trend graph
|
|
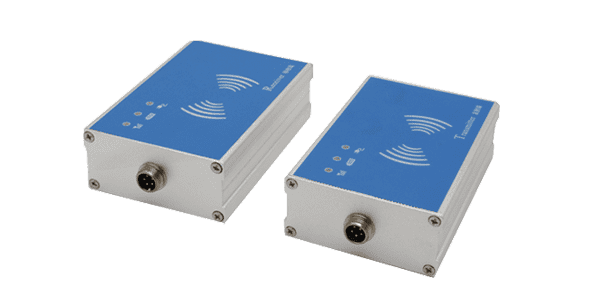
Communication
|
RS485 / Wi-Fi / Bluetooth
|
Transmits data to bedside monitor, nurse station, and hospital information system (HIS)
|
|
Power
|
Battery / AC Adapter
|
Provides excitation voltage (5–10 V DC) and system power; battery backup for transport
|
GALOCE supplies the load cell component. The A/D converter, microcontroller, display, and communication modules are typically designed by the medical device manufacturer according to their platform requirements.
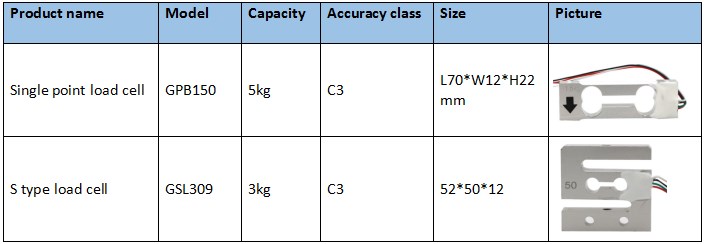
Recommended Load Cells for Urine Bag Weighing
Urine bag weighing demands a load cell with small capacity (1–10 kg typical), compact dimensions (to fit within the IV-pole mounting bracket), high sensitivity (to detect gram-level changes), and long-term zero stability (for 24/7 continuous monitoring). GALOCE recommends two micro load cell models:
|
Parameter
|
GML611
|
GML670
|
|
Type
|
Micro load cell (full bridge)
|
Ultra-thin micro load cell (full/half bridge)
|
|
Capacity Range
|
1, 2, 3, 5, 10, 15, 20, 25, 30, 40, 50 kg
|
5, 10, 20, 30, 50, 75, 100, 150, 200 kg
|
|
Material
|
Aluminum alloy
|
Manganese steel
|
|
Dimensions
|
80 × 12.7 × 12.7 mm
|
34 × 34 × 8.3 mm (ultra-thin)
|
|
Sensitivity
|
1.0 ± 0.15 mV/V
|
1.0–1.5 mV/V (full bridge)
|
|
Accuracy
|
±0.05% F.S.
|
±0.05% F.S. (full bridge)
|
|
Creep
|
±0.05% F.S. / 3 min
|
Low (manganese steel fatigue resistance)
|
|
Certifications
|
ISO9001, CE, RoHS
|
CE, RoHS, REACH
|
|
Best For
|
Standard urine bag weighing (1–5 kg range)
|
Ultra-compact integration; larger collection bags
|
|
Product Page
|
View GML611 Details →
|
View GML670 Details →
|
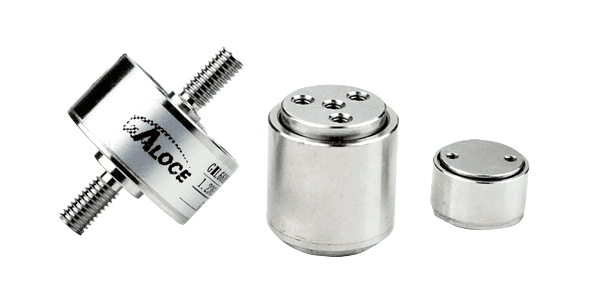
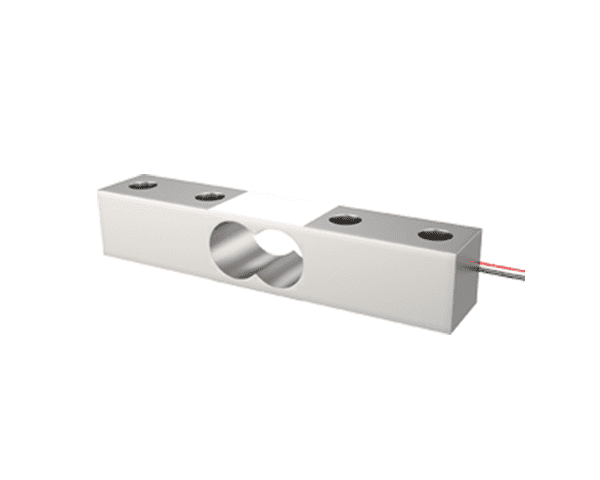
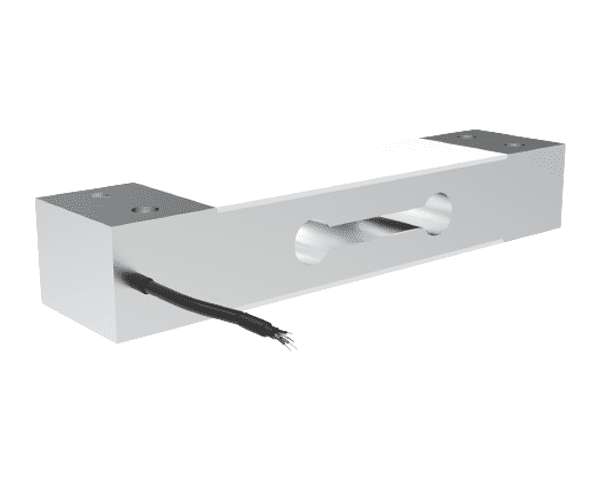
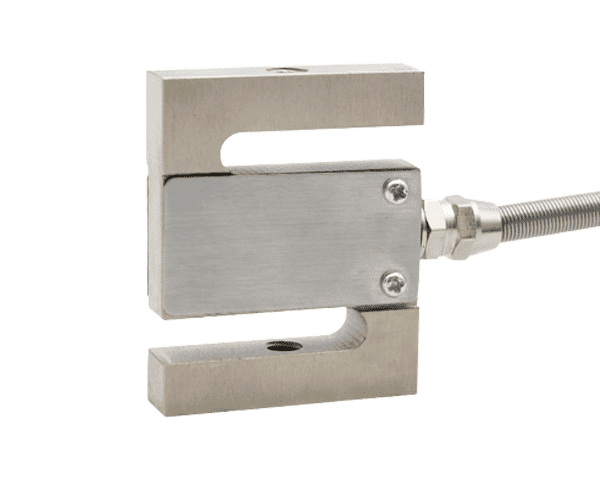
GML611 — Micro Load Cell
The GML611 is an ultra-miniature full-bridge load cell with a capacity range starting at just 1 kg — ideal for urine bag weighing where the total suspended weight (bag + urine) typically falls between 0.5 and 4 kg. Its 80 × 12.7 × 12.7 mm aluminum body is compact enough to integrate into an IV-pole mounting bracket, while the threaded mounting holes allow flexible installation angles. The ±0.05% F.S. accuracy and ±0.05% F.S./3 min creep specification ensure reliable readings during long ICU monitoring sessions. The high-quality aluminum construction provides corrosion resistance and compliance with RoHS standards.

Product Card
GML611 Micro Load Cell
Range: 1–50 kg | Sensitivity: 1.0 mV/V | Accuracy: ±0.05% F.S. | Aluminum | 80×12.7×12.7 mm
Ideal for: kitchen scales, postal scales, micro electronic weighing systems, and medical urine bag monitoring.
View Full Specifications →
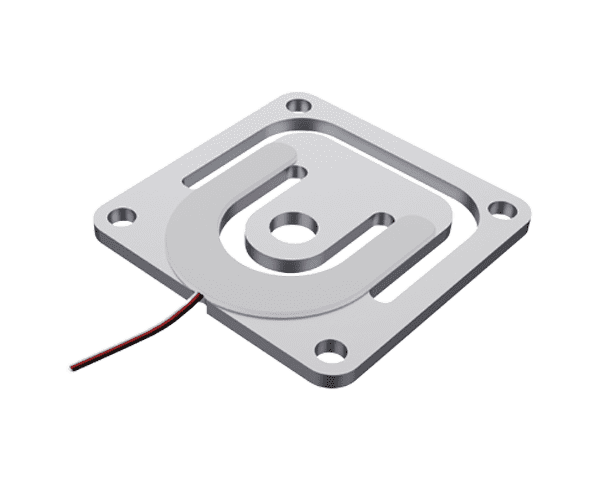
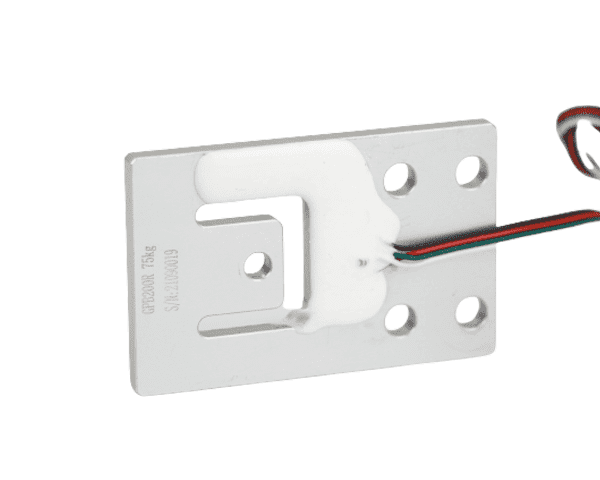
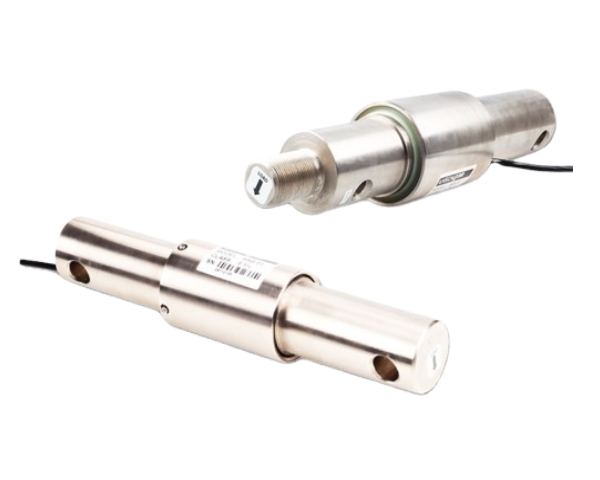
GML670 — Ultra-Thin Micro Load Cell
The GML670 is an ultra-thin micro load cell measuring only 34 × 34 × 8.3 mm — small enough to embed within the most space-constrained urine bag weighing modules. Its manganese steel construction provides superior fatigue resistance and high spring-back, ensuring the sensor returns to zero precisely even after prolonged continuous loading. Available in both full-bridge (4-wire) and half-bridge (3-wire) configurations, the GML670 offers design flexibility for different circuit topologies. The full-bridge variant achieves ±0.05% F.S. accuracy, making it suitable for clinical-grade urine output monitoring where gram-level resolution is essential.
Product Card
GML670 Ultra-Thin Micro Load Cell
Range: 5–200 kg | Accuracy: ±0.05% F.S. | Manganese steel | 34×34×8.3 mm | Full/Half bridge
Ideal for: smart scales, automated cat litter boxes, retail shelves, medical equipment, and compact urine bag weighing modules.
View Full Specifications →
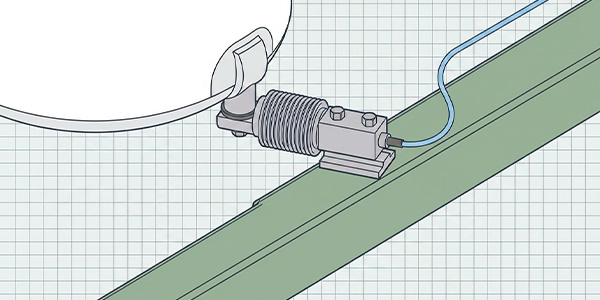
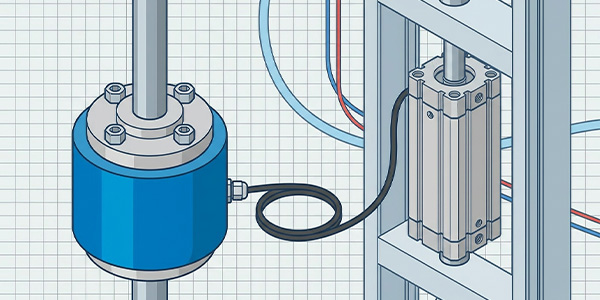
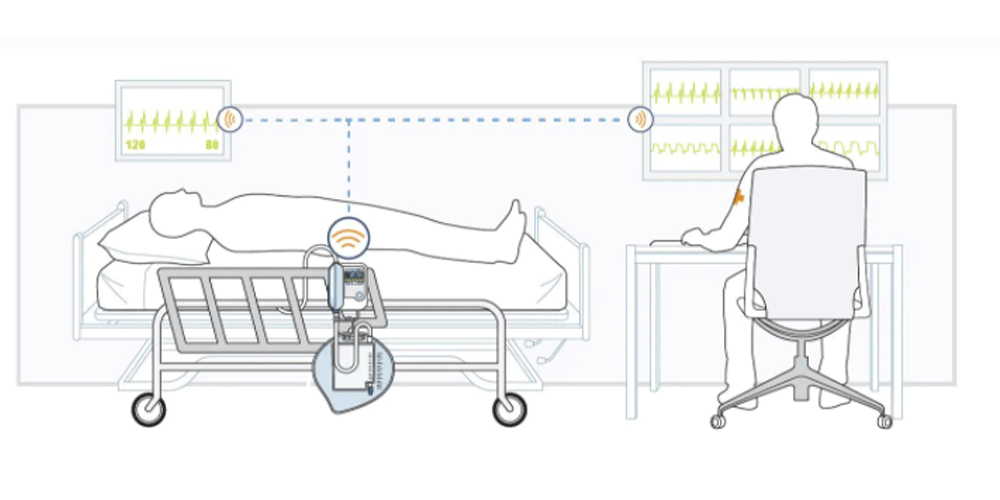
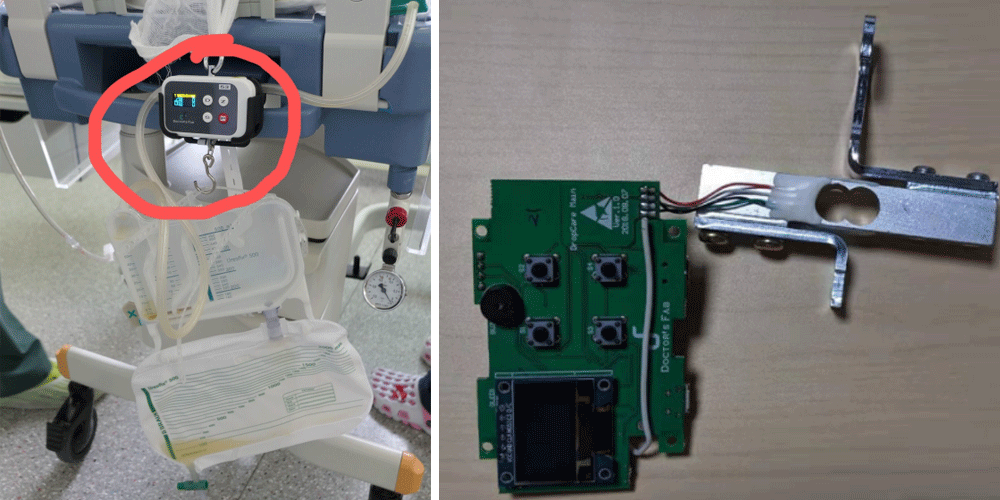
Case Study: Urine Bag Weighing Solution
The diagram below illustrates a typical urine bag weighing solution deployment. The load cell is mounted on a bracket attached to the IV pole or bed frame. The urine bag hangs from the load cell's loading point. As urine drains into the bag, the increasing weight is measured in real time, digitized by the A/D converter, processed by the MCU to calculate volume and flow rate, and displayed on the bedside monitor. Data is simultaneously transmitted to the nurse station and hospital information system.
Installation and Wiring Guide
Mechanical Installation
-
Mounting bracket: Install a rigid bracket on the IV pole or bed frame at a height that allows the urine bag to hang freely without touching the floor or bed surface.
-
Sensor orientation: Mount the load cell vertically so the loading axis is aligned with gravity. Avoid lateral forces that could introduce measurement errors.
-
Vibration isolation: Use rubber dampers between the bracket and sensor to filter out vibrations from adjustable bed motors and patient movement.
-
Cable strain relief: Secure the sensor cable to the bracket with a strain-relief clip to prevent cable pull from affecting the signal.
-
Bag attachment: Use a consistent hook or hanger for the urine bag. Variations in hook weight must be accounted for in the tare calibration.
Wiring Connections
For full-bridge load cells (4-wire configuration), the standard color code is:
|
Wire Color
|
Function
|
Connection
|
|
Red
|
Excitation + (E+)
|
A/D converter E+ terminal
|
|
Black
|
Excitation − (E−)
|
A/D converter E− terminal
|
|
Green
|
Signal + (S+)
|
A/D converter S+ terminal
|
|
White
|
Signal − (S−)
|
A/D converter S− terminal
|
For half-bridge GML670 variants (3-wire), three sensors are typically combined to form a complete Wheatstone bridge circuit. Refer to the GML670 product documentation for half-bridge wiring diagrams.
Calibration and Clinical Validation
To ensure clinical-grade accuracy, the urine bag weighing system must be calibrated before first use and re-calibrated periodically:
-
Tare calibration: With an empty urine bag and hook attached, zero the system. This establishes the baseline weight that will be subtracted from all subsequent readings.
-
Span calibration: Place a certified test weight (e.g., 1 kg or 2 kg) on the bag hanger. Verify the displayed weight matches within ±1 g. Adjust the gain in the MCU if necessary.
-
Density setting: Configure the urine density value in the system (default: 1.020 g/mL). For patients with known abnormal urine concentration, adjust the density to improve volume accuracy.
-
Flow rate validation: Infuse a known volume of test fluid (e.g., 500 mL over 30 minutes using a precision infusion pump) and verify the system's calculated flow rate matches within ±5%.
-
Periodic recheck: Re-verify tare and span calibration every 30 days, or whenever the sensor or bag hanger is replaced.
FAQ
How does the weight method convert urine weight to volume?
The system measures the real-time weight of the urine bag and subtracts the empty bag tare weight. The net urine weight is then divided by urine density (typically 1.020 g/mL) to calculate volume. For example, 1,940 g of urine divided by 1.020 g/mL = 1,902 mL. This method achieves volume accuracy within ±2%.
What capacity load cell should I choose for a urine bag?
Standard urine bags hold 1–3 liters (1–3 kg), so a 5 kg capacity load cell provides a good balance between resolution and headroom. For larger drainage bags (up to 5 liters), a 10 kg capacity is recommended. The GML611 offers capacities from 1 kg, while the GML670 starts at 5 kg.
How accurate is the weight-based urine monitoring method?
With a ±0.05% F.S. load cell and 24-bit A/D converter, the system can resolve weight changes as small as 0.5 g — equivalent to 0.5 mL of urine. This is dramatically more accurate than visual bag reading, which typically has ±10–20% error due to parallax and graduation spacing.
Can the system integrate with hospital information systems (HIS)?
Yes. The MCU can output data via RS485, Wi-Fi, or Bluetooth to a bedside monitor, which then forwards the data to the hospital information system using standard protocols (HL7, FHIR). This enables automatic charting, trend analysis, and clinical decision support without manual data entry.
What happens if the urine bag is changed or replaced?
When the bag is changed, the system should be re-tared with the new empty bag attached. Many systems include an automatic "bag change" function that records the cumulative output before the swap, resets the tare, and continues monitoring from zero — ensuring no data is lost during the exchange.
Is the load cell affected by temperature changes in the hospital room?
Both GML611 and GML670 include temperature compensation. In typical hospital room temperatures (18–25 °C), the zero drift is negligible. For environments with wider temperature variation, the MCU can apply software temperature correction using a built-in thermistor reading.
Related Topics